
Summaries by Nathan Elliott. Formatting and editing by Madeline Rizzo
| Day One Summary | Day Two Summary | Day Three Summary |
|---|

The Strategic Health Information Exchange Collaborative (SHIEC) is a national collaborative that represents health information exchanges (HIEs), associated organizations, and strategic business & technology partners.
2021 marks the seventh year of SHIEC! We are excited to be both back in person and viewing the sessions virtually. Join us over the upcoming days as we recap selected sessions from this year’s events!
A Discussion with the 21st Century Cures Champions

- Date: Wednesday, August 18, 2021
- Presenters:
- Representative Diana DeGette (D-CO)
- Representative Fred Upton (R-MI)
- Lisa Bari, Interim CEO, SHIEC
- Overview: Representatives Diana DeGette (D-CO) and Fred Upton (R-MI) join Lisa Bari, CEO of SHIEC, for a discussion about their previous roles in passing the 21st Century Cures Act and their efforts to update this legislation before the end of 2021 with “Cures 2.0.” DeGette and Upton describe what they feel contributed to success in securing strong bipartisan support for the Cures Act and what they are doing to repeat that success with this year’s important update.
In 2015, Representatives DeGette and Upton successfully moved the 21st Century Cures Act through Congress. According to DeGette, the Cures Act was intended to modernize how the country discovers, develops, and delivers groundbreaking solutions in healthcare.
She described the Cures Act as the most comprehensive legislation of its kind since the Affordable Care Act. The intent was to get better at screening and preventing certain types of cancer, better understand the human brain, and advance regenerative medicine. The Cures Act proved to be successful, enhancing data sharing and putting patients more at the center of their care with greater access to and control over their health information.
Rep. DeGette said that the next iteration is meant to help us remain at the cutting edge and take advantage of developments in virtual care, expanded data sharing, and ensuring supply chain sufficiency and availability for public health emergencies.

Rep. Upton talked about the importance of the level of bipartisan support that they had during the original Cures Act process. He recognized that topics such as disease tend not to be party-specific and certainly make it easier to find support all around. These are human issues that affect all of us, regardless of political affiliation or agendas. Cancer does not care about on which side of the aisle someone sits.
Just like the rapid development of COVID-19 vaccines, pushing through major legislation requires a large network of relationships and partnerships. Rep. Upton expects to continue the approach of investing considerable time hearing from stakeholders representing as many aspects of healthcare research, planning, and delivery as possible.
Rep. DeGette explained that discussions were not always easy when experts disagreed on facets of the proposed legislation or solutions. When any impasses arrived, however, the authors elected to table that topic to discuss what people agreed on instead.
Upton and DeGette have issued multiple discussion documents over the past year and have received over 500 comments on the new proposed updates. Even though submission deadlines have passed, Upton and DeGette are still listening and want to hear from as many groups and stakeholders as possible that are willing to share their voices.
DeGette added that COVID-19 really highlighted the importance of data sharing and data sharing infrastructure. They expect to include these topics in this year’s Cures 2.0 legislation. New directives should help to guide national strategies based on lessons learned from the pandemic. DeGette specifically invited listeners to offer suggestions on where proposed language could be stronger.
On the topic of virtual care, DeGette said that Cures 2.0 will certainly include provisions to make telemedicine permanent for a number of situations and its appropriate use. However, she cautioned that it will not force a change to the customary model of seeing a doctor.
The session ended with both speakers relaying examples of disparities that still need to be addressed and are contemplated in Cures 2.0, both rural and urban.
Rapid Innovation and New Partnerships


- Date: Wednesday, August 18, 2021
- Presenters:
- Lisa Bari, Interim CEO, SHIEC
- Kate Ricker-Kiefert, Consultant, Strategic Health Information Exchange Collaborative (SHIEC)
- Jolie Ritzo, Director, Partnerships & Programs, Network for Regional Healthcare Improvement
- Perry Ellington, Director, Solution Architecture & Clinical Services, The Health Collaborative
- Tiffany Mattingly, Vice President, Clinical Strategies, The Health Collaborative
- David Hartley, Associate Professor of Pediatrics, University of Cincinnati School of Medicine
- Emily Hartmann, Executive Director, PHIX
- Rhonda Spellmeier, HIE Workflow Specialist/Nurse Informaticist, KHIN
- Felicia Quintana-Zinn, Nebraska Department of Health and Human Services
- Angela Greene, Director, CyncHealth
- Christie Burris, Executive Director, North Carolina Health Information Exchange Authority
- Eric Myers, Principal Technical Consultant, SAS Institute
- Carolyn Stone, Director of Operations, VITL
- Overview: In this session, presenters provide short summaries of a variety of HIEs’ rapid response efforts during the COVID-19 pandemic to produce valuable tools and services to government partners.
North Carolina HealthConnex is a state-designated HIE covering more than 7,000 facilities, including 130 hospitals across the state. HealthConnex was established in 2016 as part of a public-private partnership with SAS Institute as the hosting and technology partner. Like other HIEs across the country, HealthConnex responded to the COVID-19 pandemic with a series of services:
- Integration of visit data to the NC syndromic surveillance system for monitoring statewide trends for COVID-like illness
- Integration of HealthConnex with state reportable lab system to store and forward COVID-19 results to providers using a subscription-based event notification service
- Real-time patient-level business intelligence for NC Medicaid to drill into geographic data and follow patient-specific disease progressions
- Patient matching and data delivery services for vaccine reporting to the NC Department of Public Health’s COVID vaccine management system
 Since there was no single source for reportable labs for COVID, HealthConnex partnered to bring results into the HIEs. HealthConnex stood up a lab feed from the Department of Public Health. This feed was essential to the BI reports that were prototyped in early 2020.
Since there was no single source for reportable labs for COVID, HealthConnex partnered to bring results into the HIEs. HealthConnex stood up a lab feed from the Department of Public Health. This feed was essential to the BI reports that were prototyped in early 2020.
As vaccines began to roll out, the state analyzed their IIS system and determined that it would not be scalable enough to onboard providers. NC tapped their HIE to help with data connections into a new system and leveraged patient matching. The state’s COVID-19 management system was ultimately based on HIE routing.
—
PHIX, which serves the El Paso, TX region, reported the following about their COVID-19 response:
- 137,000 electronic COVID-19 lab orders and results facilitated by PHIX
- 49,000 COVID-19 results sent securely to individuals by email or text
- 140,000 COVID-19 case investigations tracked and supported electronically
- 600 patient transfers to alternate hospitals supported during COVID-19 hospital surge
- 221,000 COVID-19 vaccinations reported electronically to the Texas immunization registry
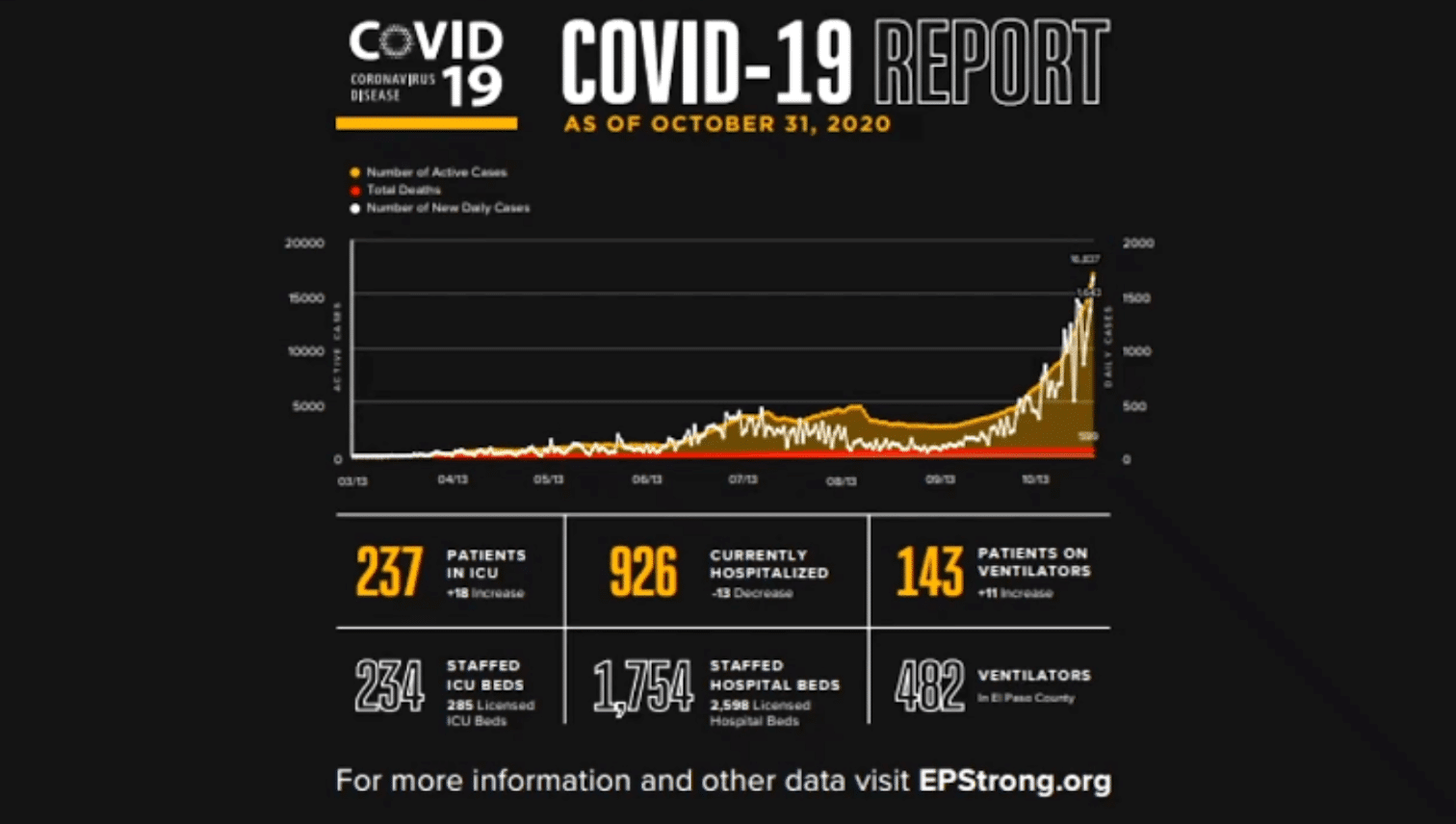 In October 2020, El Paso set up an alternate site for patient transfers due to ICU bed scarcity. PHIX was directly involved in helping to save time during the nearly 300 transfers that took place to the temporary site. In other communities, transfers required faxing or securely pushing medical records and could take hours for approval. In El Paso, PHIX extended their clinical viewer portal to the temporary care site for care team members to review real-time patient data from PHIX. The approval process took less than 10 minutes.
In October 2020, El Paso set up an alternate site for patient transfers due to ICU bed scarcity. PHIX was directly involved in helping to save time during the nearly 300 transfers that took place to the temporary site. In other communities, transfers required faxing or securely pushing medical records and could take hours for approval. In El Paso, PHIX extended their clinical viewer portal to the temporary care site for care team members to review real-time patient data from PHIX. The approval process took less than 10 minutes.
PHIX also leveraged its data to help identify patients in standard hospital ICU beds who might be candidates to transfer to the Beaumont Army Medical Center, which had available beds because they could only accept service members. Nearly 300 patients were ultimately transferred to Beaumont, taking pressure off other ICU beds for the general population.
After the initial response to COVID-19, PHIX developed the Vaccination Information Exchange (VIX), which facilitates electronic reporting to the state’s registry and driver’s license scanning to collect more complete demographic information in support of the region’s walk-up vaccination model. PHIX was able to put in place an important safety check prior to vaccination administration to ensure that the individual was not already vaccinated, had not had recent infusions, was not currently COVID-19 positive, and that the vaccine was generally safe to give the individual at the time of administration. PHIX is currently working on supporting booster administrations.
—
Vermont Information Technology Leaders (VITL) responded to the pandemic early on by convening the following:
- VITL’s clinical data architect, application systems analysts, interface engineers, database administrators, and support and leadership
- Vermont Department of Health’s epidemiology team
- Vermont Department of Health’s data analysts and project managers
- Members of the Vermont State Emergency Operations Center (SEOC)
- Hospital clinical and technical teams
 These teams worked to define COVID-19 reporting criteria and built an initial report. To improve data quality, VITL worked with hospitals to standardize ICU bed indicators. The HIE also worked quickly to add COVID-19 testing lab interfaces. These improvements allowed the prototype report to be refined over approximately a two-month period. This data has continued improving as VITL works with hospital teams to further enhance the data through automated data capture or lab data normalization through terminology technology.
These teams worked to define COVID-19 reporting criteria and built an initial report. To improve data quality, VITL worked with hospitals to standardize ICU bed indicators. The HIE also worked quickly to add COVID-19 testing lab interfaces. These improvements allowed the prototype report to be refined over approximately a two-month period. This data has continued improving as VITL works with hospital teams to further enhance the data through automated data capture or lab data normalization through terminology technology.
The COVID-19 report ran daily, and VITL leveraged APIs to send specific data to the State Emergency Operations Center’s daily tracking dashboard. VITL included automated state-mandated reporting, which eliminated two separate reporting burdens for hospitals and is still in effect today.
In order to accomplish the construction of these reports, VITL obtained legal authorizations early on with help from Health and Human Services (HHS) and the Vermont Agency of Health and Human Services (AHS), as well as reached an agreement from participating hospitals to engage in this work and share needed data.
VITL shared the following lessons learned:
- Short collaborative implementation iterations worked best, as the nature of the crisis response changed rapidly.
- Gathering teams from all sides on working calls to analyze data quality in small increments helped to identify and solve issues more quickly.
- Aggregated data from across the community produced more accurate data.
- Data sharing agreements and getting new tests and codes in place takes time.
- Having existing infrastructure, the right people in place, and support from all levels of the state, including the governor, were key.
—
At the time the pandemic emerged, the Kansas Health Information Network (KHIN) had 97% of hospitals in the state connected and contributing data to the HIE. KHIN put a dashboard solution they already owned in use and stood up a COVID-19 reporting tool in about six weeks.
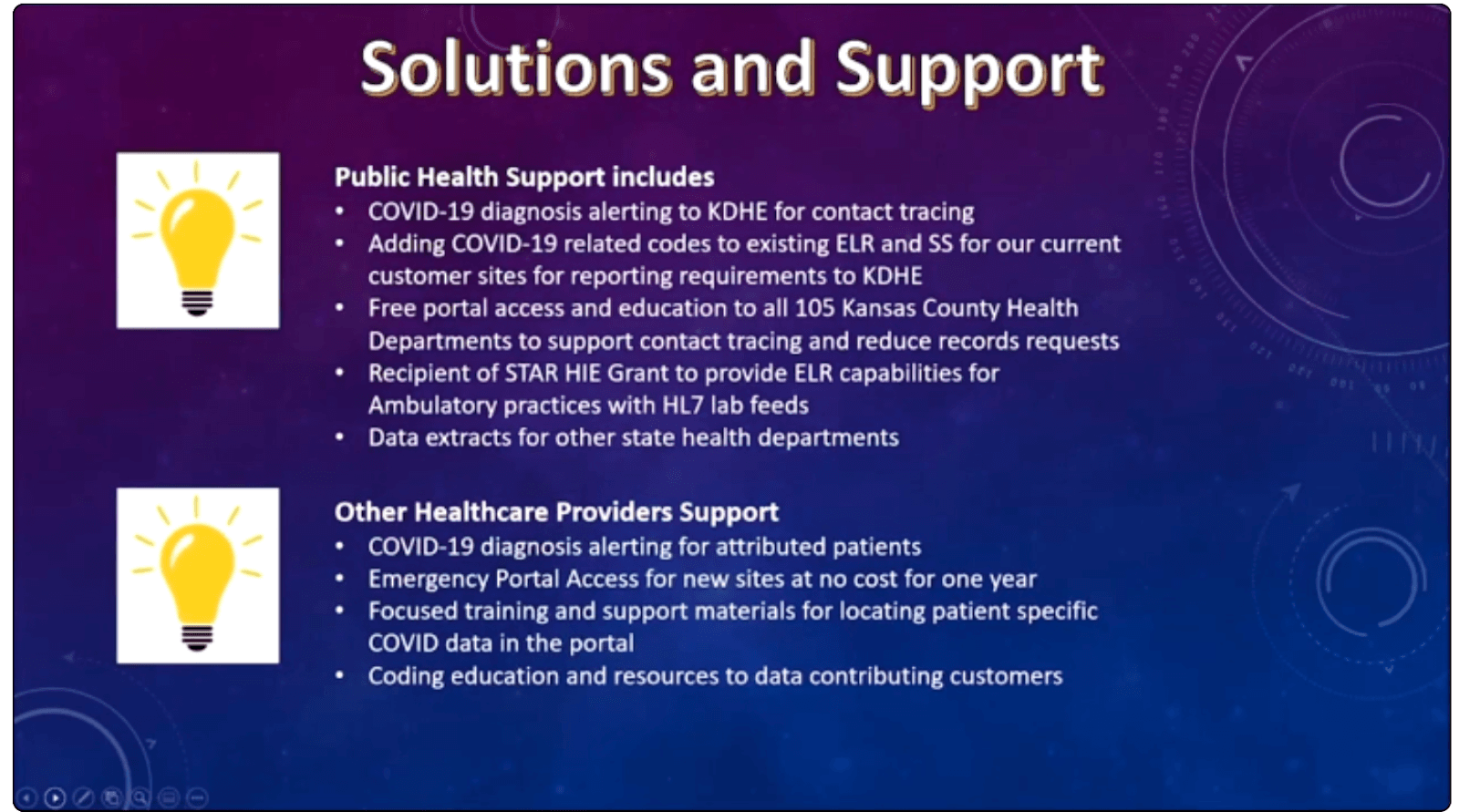 KHIN also developed and deployed the following:
KHIN also developed and deployed the following:
- COVID-19 diagnosis alerting to the Kansas Department of Health and Environment for contact tracing
- COVID-19 related codes to existing Electronic Lab Reporting (ELR) and Syndromic Surveillance (SS) for mandatory reporting
- Free portal access and education to all 205 Kansas County Health Departments to support contact tracing and reduce traditional record requests
- ELR capabilities for ambulatory practices with HL7 feeds
- Data extracts for other state health departments
- COVID-19 diagnosis alerting for providers for attributed patients
- Emergency portal access for new sites at no cost for one year
- Coding education and resources for participants contributing data
KHIN is continuing to refine the information available in their portal to benefit the HIE’s multiple stakeholders.
—
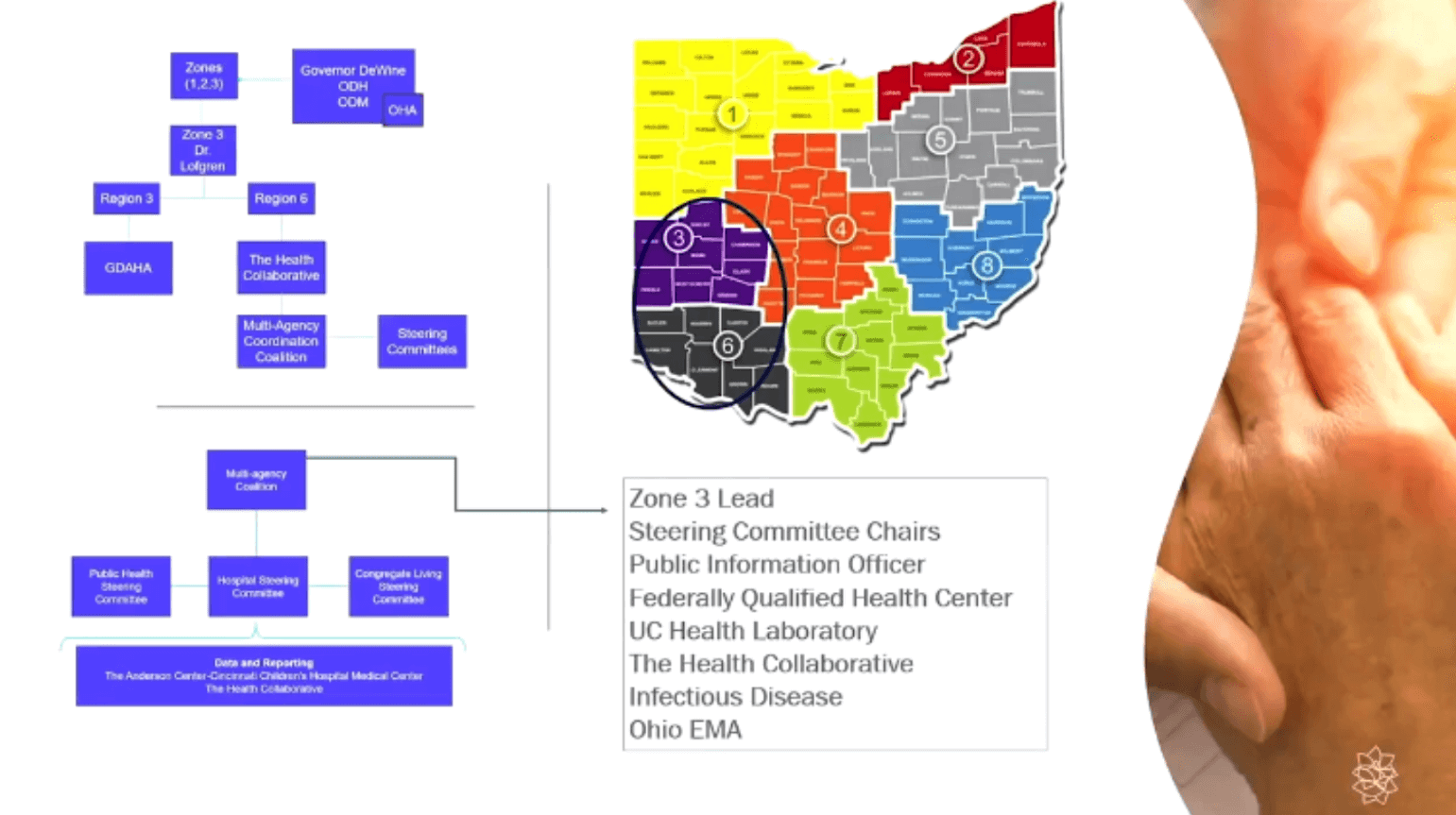 In addition to COVID-19 tracking dashboards, The Health Collaborative developed a model to forecast COVID-19 surges and sent this information to decision-makers. They worked with data scientists, epidemiologists, and a physician to review information daily and discuss implications.
In addition to COVID-19 tracking dashboards, The Health Collaborative developed a model to forecast COVID-19 surges and sent this information to decision-makers. They worked with data scientists, epidemiologists, and a physician to review information daily and discuss implications.
The model helped to inform a surge escalation plan, which 34 hospitals agreed to use. This plan helped manage resources, such as personal protective equipment (PPE), elective procedure schedules, ventilators, and transfers. Hospitals used a combination of data and their experience to make these decisions.
—
Nebraska’s CyncHealth identified limitations with contact tracing systems. CyncHealth took advantage of relationships between organizations to find better solutions. The goal was to provide comprehensive contact tracing for as long as possible. CyncHealth worked with the state over a 12-week period to develop a finished solution for enhanced contact tracing, and an initial 1,000 users were onboarded within two weeks of go-live.
 CyncHealth is continuing to innovate and perfect this new system. They have employed fast-paced iterations and have relied heavily on the trust and respect they have nurtured with the state prior to the pandemic.
CyncHealth is continuing to innovate and perfect this new system. They have employed fast-paced iterations and have relied heavily on the trust and respect they have nurtured with the state prior to the pandemic.
CyncHealth believes that a team approach and having proactive discussions about future collaborations and innovations will establish the foundation for rapid collaborative responses to urgent needs.
Some of the presenters provided some final words of advice:
- Contracting language can take a while to work through. Set up agreements in advance with broad and flexible wording to enable rapid responses and resource sharing.
- Contact partners as early as possible when threats emerge. Waiting a few weeks can have direct implications for rapidly changing and growing threats.
- Be ready to partner on things that your organization or team might not be a complete fit for. Partnerships and shared responsibility are critical to rapid response success.
- Responses are most effective when technology, data, agreements, community partners, and the right talent are in place or accessible. It is a good idea to ensure these elements are accounted for before an emergency.
- Working relationships tend to be better, and results come faster, when HIEs truly listen to their partners in the community and enter conversations with a mindset of service to others.
The Evolution of Clinical Data Access in HIEs
- Date: Wednesday, August 18, 2021
- Presenters:
- Tom Moore, Senior Vice President, Innovation, Healthix
- Mike Bouton, CMIO, New York Health + Hospitals
- Nick Ramsing, Director of Product Development, CRISP
- Overview: CRISP and Healthix offer details about a new embedded HIE data viewer that works with Epic and other EHRs. Presenters talk about the limitations of other information delivery mechanisms for providers and discuss what’s next for this new technology.
The presenters open their discussion by providing audience members with brief backgrounds about their respective organizations. Healthix serves New York City and surrounding areas. CRISP serves Maryland and Washington DC, as well as provides shared services for a growing number of HIEs and clients in other states. NYC Health + Hospitals, finally, is an integrated healthcare system of hospitals, neighborhood clinics, long-term care facilities, nursing homes, and home care. It is the largest public health system in the country and is the safety net system of New York City.
The session included examples of Dr. Bouton’s success with making better decisions in an Emergency Department within the NYC Health + Hospitals system. One example includes pediatric and adult patients for whom having access to Healthix data changed the severity of treatment Dr. Bouton considered. In one case, a child came to the ED with very rapid breathing and a large scar on their chest, but no other information. Dr. Bouton was able to pull information from a health system outside of the NYC Health + Hospitals system to learn the child’s history. He then understood he was likely treating the child for a cold instead of some major condition.
Presenters also discussed the history of accessing clinical data through HIEs. In the past, the primary mode was through a stand-alone clinical viewer. While these viewers are available to any qualified provider with appropriate access, they do not fit easily into providers’ workflows. In addition, they also require additional clicks and usernames/passwords. Many providers are not interested in relying on another website with separate credentials to remember and enter each time they need information. Clinical viewers can also provide “too much” information for any given provider or specialty.
Single Sign-On technology can improve clinical viewer tools by helping providers launch out of a system, like an EHR, to the clinical viewer, but implementation has been complicated. The next option is for providers to be able to query for documents through their EHR. The problem with this model is that the user experience is unpredictable. In some cases, perhaps a single document returns. In another situation, dozens might return, requiring the provider to click into individual documents to search for the information they need.
 Another option is a bulk export of HIE data (discrete or parsable). While this option does provide greater flexibility in determining which data to use and display, such as within an EHR, the HIE loses control of the user experience.
Another option is a bulk export of HIE data (discrete or parsable). While this option does provide greater flexibility in determining which data to use and display, such as within an EHR, the HIE loses control of the user experience.
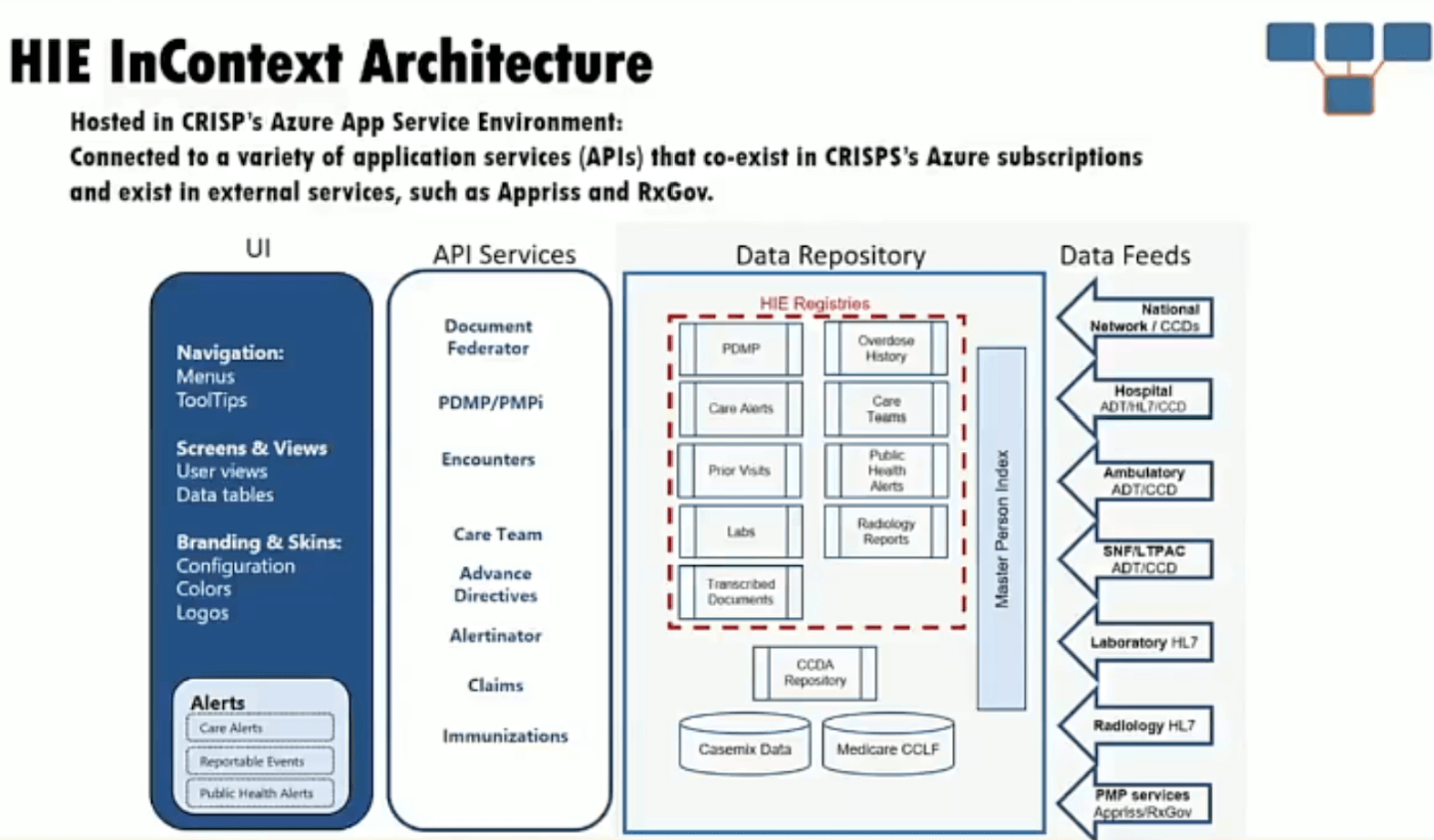
To respond to the limitations of these primary options for information delivery, CRISP has developed an application that embeds HIE data in the EHR so that it is both managed by the HIE and is made part of the clinician’s existing workflow.
The tool has been branded InContext and is complementary to exchange tools like Epic’s Care Everywhere. Features include:
- Patient matching
- Medication management (PDMP advisories and medications)
- Health records and encounters, structured documents, and immunizations
- Advance directives
- Social determinants of health assessments and referrals
- Claims data
- HIE portal launch
- Alerts for specific types of information such as care alerts, medication, and infection control
InContext has been deployed to over 30 health systems, primarily in Maryland and DC, but with adoption growing elsewhere. Today, InContext enjoys over 90,000 launched sessions per week. The most-used screens are PDMP and patient health records.
Healthix is now leveraging this technology from CRISP to deploy for member hospitals in New York. Healthix has re-branded its version of the embedded application as Healthix Concise. Healthix is now in the process of rolling out the application to Epic sites. Other EHR integrations are also available.
Future considerations include:
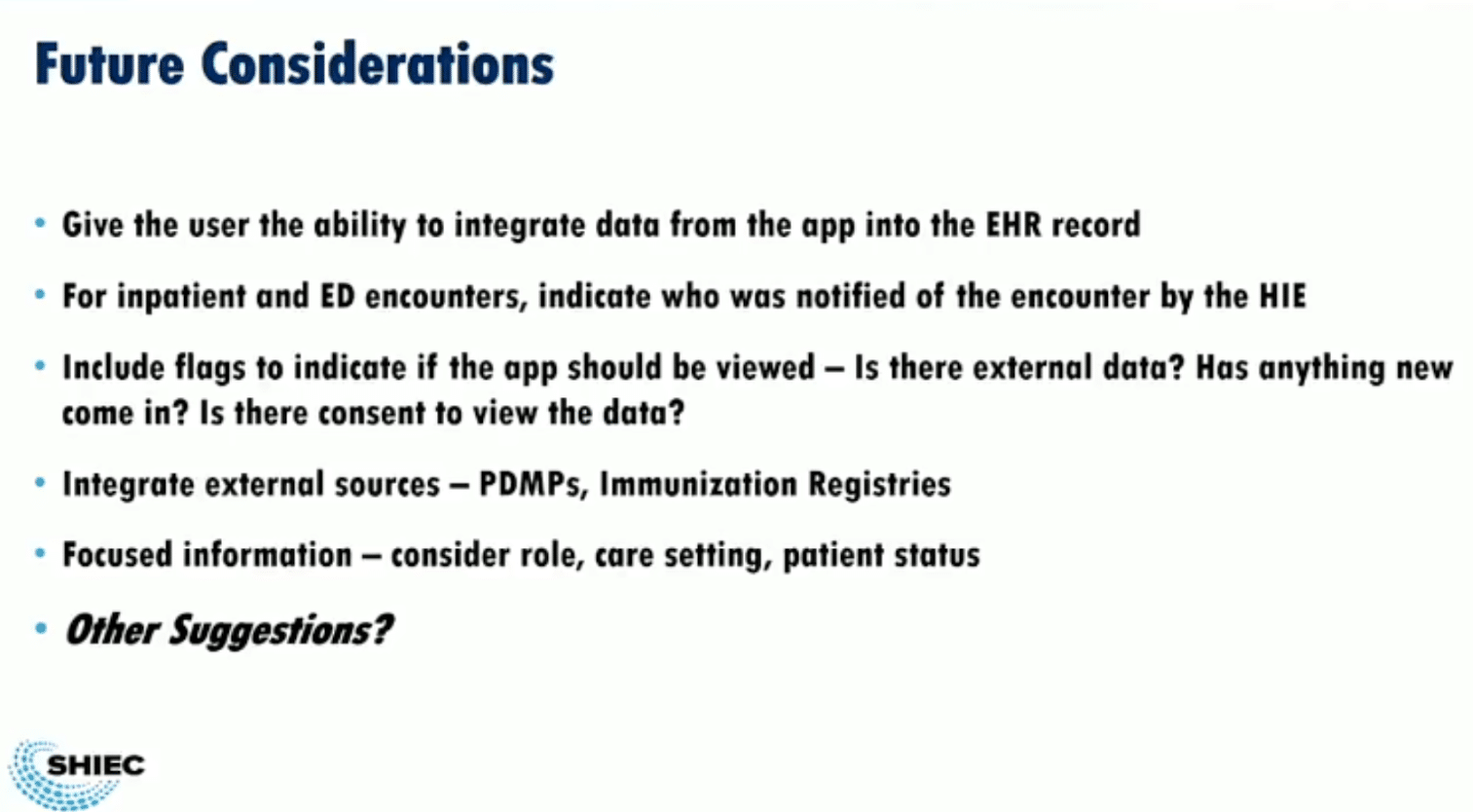
- The ability for providers to incorporate data from the application back into the patient record (today, it is display-only)
- The ability to indicate which care team members were notified of the encounter by the HIE for inpatient and ED encounters
- The inclusion of flags to help determine whether the app should be opened, such as new external data, updated consent, etc.
- The integration of external sources, such as PDMP and registries
- Focused information by provider or specialty
Presenters and audience members discussed future needs such as customizing data by specialty—assuming a hospital can arrive at a consensus about what to display by specialty and whether this would meet all providers’ needs.
At this time, Epic is not charging for the use of this application, but presenters did anticipate charges in the future from other EHRs. So far, the HIEs have not opted to pass those costs on to hospitals. Fees will need to be examined going forward.
Certified Use of HIE Data to Support Multi-Payer Quality Measurement Programs

- Date: Wednesday, August 18, 2021
- Presenters:
- Dan Porreca, Executive Director, HEALTHeLINK
- Sarah Cotter, Director of Client Engagement and Population Health, HEALTHeLINK
- Wendy Talbot, Assistant Vice President, Measure Collection & Audit, NCQA
- Overview: HEALTHeLINK’s Dan Porreca and Sarah Cotter discuss their experience piloting NCQA’s data aggregator certification program as part of an early cohort last year. Lessons learned could help HIEs planning to go through their own NCQA certification to support payers with HEDIS reporting and audits. NCQA’s Wendy Talbot shares her perspective on the certification process and pertinent updates to requirements, as well as NCQA’s timeline for the coming months.
HEALTHeLINK operates in western New York state and features the following:
- 100% participation of western New York hospitals
- More than 90% of western New York practices participating with 6,500 providers
- 90% of the western New York population consented to participate
- Nearly 100% of lab results available
- More than 90% of radiology reports available
- Images from more than 20 radiology facilities available
- Claims data from health plans representing 70% of covered lives in western New York
- More than 500 data sources

HEALTHeLINK identified years ago that the HIE should serve public health purposes and saw opportunities in developing quality measures based on the combination of clinical and claims data. HEALTHeLINK had been sending CCDs to health plans for at least five years, but these CCDs were only a single view (not comprehensive) and could not be used as standard supplemental data (primary sources were still needed). Now, years later, HEALTHeLINK sees important new opportunities in NCQA’s Data Aggregator Validation (DAV) program to lessen the burden of audits for its partner health plans.
Wendy Talbot, Assistant Vice President, Measure Collection & Audit for NCQA, presented background information about the DAV program. The problem that NCQA wanted to solve was a combination of the following: that the audit burden for HEDIS was quite high, decisions were not transportable, technology and information “hubs” had evolved and matured, but there was still variability in CCDs, and they were not consistently implemented.
NCQA sought to develop a program like HEDIS audits for health plans but for clinical data aggregators. NCQA approached the state of New York for funding support, and in fall 2019, they contracted to begin with three HIEs. The goal was to validate data from ingestion to output at the HIE (or data aggregator) level once and reduce the burden of audits, which often required direct support from potentially hundreds of primary data sources.
NCQA’s DAV program is now live. The validation process kicked off with the first regular cohort on July 26, 2021.
Talbot listed the following expectations for data aggregators:
- Complete Validation Assessment Tool (VAT)
- Virtual review participation
- CCD conformance on synthetic and real data tests (using synthetic data might become optional)
- Corrective actions submissions, if applicable
Aggregators will be required to pass both the input data validation and the output file validation in order to be considered validated. Once validated, aggregators can share validated data sources as standard supplemental data for HEDIS reporting without additional auditing needs.
 Talbot further clarified that samples are used for a given cluster of sites. Once validated (e.g., 100 sites), those sites would not need to be validated again during the annual recertification process. If the cluster grows, however, samples of the delta might need to be validated. The second official cohort of data aggregators is expected to begin their validation process in October of this year.
Talbot further clarified that samples are used for a given cluster of sites. Once validated (e.g., 100 sites), those sites would not need to be validated again during the annual recertification process. If the cluster grows, however, samples of the delta might need to be validated. The second official cohort of data aggregators is expected to begin their validation process in October of this year.
HEALTHeLINK’s Sarah Cotter took the podium and presented information about the HIE’s efforts to improve data quality, both for NCQA purposes and for general use. In 2020, HEALTHiLINK hired a data quality manager to work across departments and analyze physician/provider data, coding accuracy, and population health metric validation. The data quality manager developed tools to help understand the quality of the data coming into the HIE. Part of the effort to track data quality included such details as when participants were expected to take EHR upgrades to monitor for changes.
The HIE formed a data quality committee focused on New York State DQIP and a sub-committee with external stakeholders, each of which met bi-monthly. The latter worked on projects, including LOINC code mapping, which boasted a 50% improvement in just a few months, and monitoring scorecards developed for data quality improvement to target outreach and coordination efforts.
HEALTHiLINK also developed a tool called Inspector of Health Care Quality (iQHD). This tool analyzes the quality of C-CDAs received by section (or category) based on a defined rule set and yields a data quality report. The tool and accompanying report help to identify areas for improvement. Some issues are related to data entry, and some are vendor-related. Future versions are expected to provide a way for stakeholders to compare their scores against those of the group of participants.
The HIE aligned these tools and reports to the NCQA DAV program. The output scorecard provides the ability to drill into detailed error descriptions to help office managers understand where data is missing in documents. Teams can monitor these DAV-aligned displays over time to spot sudden changes as well as verify improvement efforts.
As part of the NCQA validation process, HEALTHeLINK worked through primary source verification (PSV). The original methodology included a sample from all data sources (225+ for HEALTHeLINK). Based on experience and feedback, they moved to an EMR cluster approach to get a sample of 50 total primary sources. This required screenshots from EMRs to verify inbound ingested CCD XML and then comparing these screenshots to outbound aggregate CCD XML from the HIE to ensure they matched.
In addition to the DAV program, HEALTHeLINK initiated a project to send aggregate CCDs of all certified data to local payer partners for standard supplemental HEDIS reporting. The HIE worked with charter payer partners to define a two-year historical lookback period for these CCDs and the intended frequency of distributing them. In June of 2021, HEALTHeLINK began generating historical CCDs with certified data. In October 2021, HEALTHeLINK plans to begin weekly document distribution. The health plans are currently working on ingesting these CCDs.
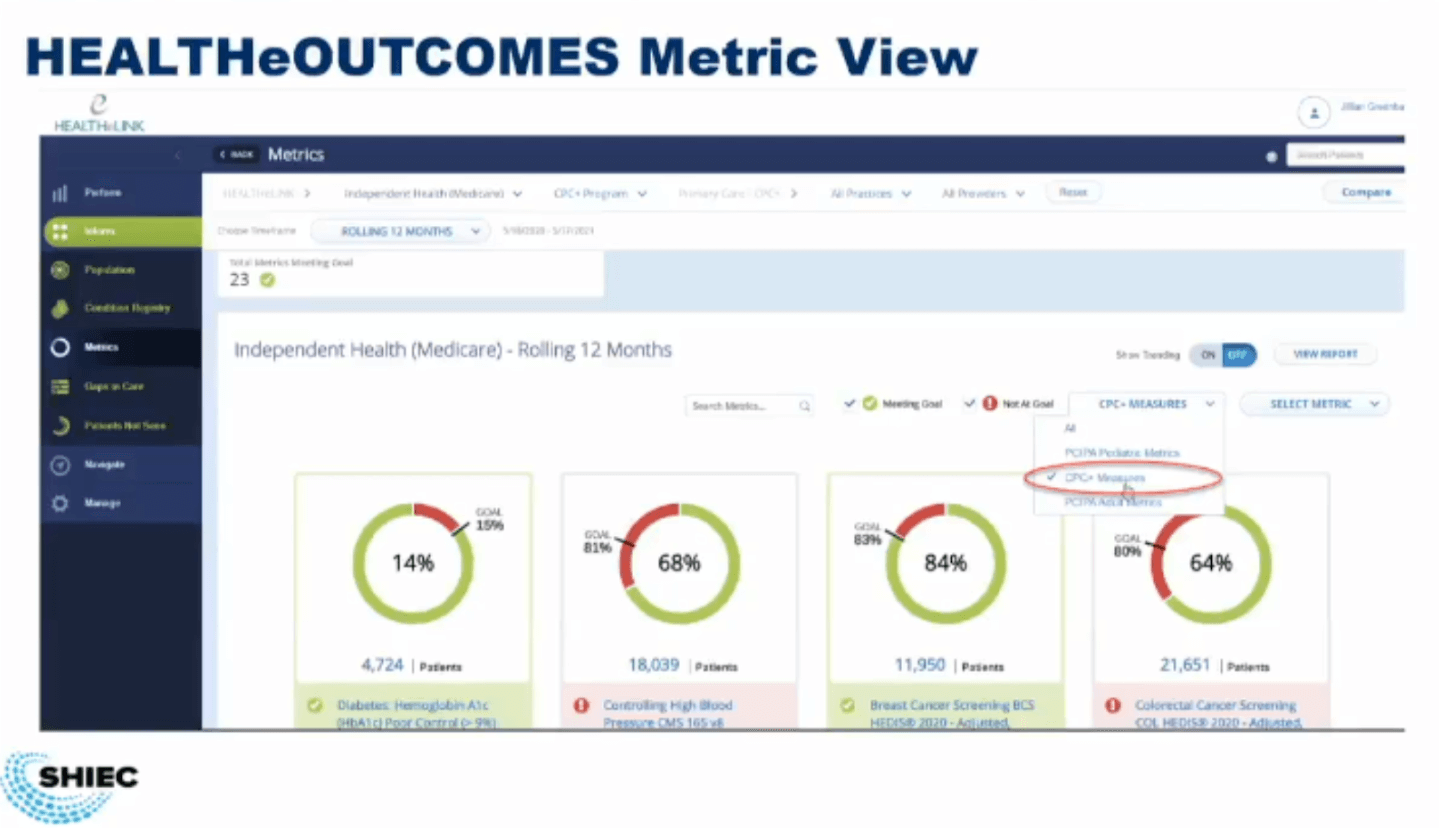 Taking all of this a step further, HEALTHeLINK partnered with NextGen Healthcare to offer a population health tool to the western New York market, which was branded HEALTHeOUTCOMES. The solution blends clinical and claims data for patients and presents a visualization that includes gaps in care, quality metrics, and risk scores to improve care and better manage value-based purchasing.
Taking all of this a step further, HEALTHeLINK partnered with NextGen Healthcare to offer a population health tool to the western New York market, which was branded HEALTHeOUTCOMES. The solution blends clinical and claims data for patients and presents a visualization that includes gaps in care, quality metrics, and risk scores to improve care and better manage value-based purchasing.
HEALTHeOUTCOMES gives payers and health systems agnostic snapshots of common quality measures across payer contracts. The solution stratifies patient panels by age, gender, and several standard risk models (i.e., ACG, HCC, ASCVD).
The HEALTHeLINK team provided the following advice to organizations planning to pursue the NCQA DAV program:
- Plan for 1-2 FTEs of dedicated focus on NCQA for approximately 18 weeks.
- Factor costs into budgets for annual recertification.
- Be open with NCQA and provide as much feedback as possible. Much of this is learning together to improve the certification process.
Wendy Talbot stated that annual recertifications are likely to focus primarily on “what has changed” since the last certification. Clusters that were certified previously will not need to be recertified unless there are significant changes. The recent process will likely begin with a self-assessment to determine what changes have occurred since the previous year. NCQA will then focus on those, making recertification an abbreviated version of the initial validation process.
Thank you for joining us for day three at SHIEC! Until next year!
| Day One Summary | Day Two Summary | Day Three Summary |
|---|
J2 Interactive is an award-winning software development and IT consulting firm specializing in customized solutions for hospitals, labs, research institutions, and health information exchanges.
Our approach to design and development is rooted in a fundamental belief that systems succeed or fail based on how well they serve the people who depend upon them. Drop us a line to learn more.