
| Week Two Summary | Week Three Summary | Week Four Summary | Week Five Summary |
|---|
2020 marks the sixth year of SHIEC and the first year of it going virtual! Join us over the next five weeks from August 17 – September 15 as we recap the 10-day series of virtual sessions!
Welcome & Opening Remarks

- Date: Monday, August 17, 2020
- Presenters:
- Melissa Kotrys, MPH, CEO, Health Current, Chair, SHIEC Board of Directors
- Kelly Hoover Thompson, CEO, SHIEC
- Overview: Melissa Kotrys and Kelly Hoover Thompson open 2020 SHIEC by discussing what the presentations will cover, events that will be going on, and where SHIEC will be held in the upcoming years.
The work HIEs do has never been more critical, and Melissa Kotrys and Kelly Hoover Thompson emphasized this sentiment in their 2020 SHIEC Welcome & Opening Remarks. With the COVID-19 pandemic, HIEs have become even more visible at the state level, as well as nationally. We have seen a unique sense of urgency among public health agencies and provider communities to rally around the work that HIEs are doing to facilitate more useful, accurate, and coordinated insights into disease tracking and response effectiveness. The current pandemic has been a catalyst for accelerating HIE awareness and engagement for near-term problem-solving, but HIEs must continue to seek breadth and agility in their solutions and outreach. A single pandemic can be a critical inflection point for an HIE to demonstrate its place in the information sharing ecosystem, but there are still many other local and national health challenges that need our attention.

In laying out the agenda for 2020 SHIEC, Thompson explained that each of the conference sessions will cover examples of various HIE approaches during the pandemic and new policies that will affect HIEs in the future.
In addition, she mentioned there will be other activities going on, such as a selfie program, virtual exhibits (visit J2’s booth!), a scavenger hunt, and multiple $100 gift card drawings.
Look for information online about joining SHIEC and its members and supporters in Scottsdale, AZ, in August of 2021 and San Antonio, TX, in August of 2022.
Mark your calendars!
Opening Keynote

- Date: Monday, August 17, 2020
- Presenter: Adi V. Gundlapalli, MD, PhD, MS, Chief Public Health Informatics Officer at the Center for Surveillance, Epidemiology, and Laboratory Services (CSELS), Centers for Disease Control and Prevention (CDC)
- Overview: Dr. Gundlapalli highlights the key areas of value provided by HIEs in a world of quickly evolving data and changing information needs.
Public health response begins with good data. Increasingly, local, state, and national agencies are looking to programs to provide disease and population insights for not only policy-making and planning but also real-time public health emergency response. We have been building infrastructure for years and are now beginning to see those investments pay off. Because SHIEC covers 95% of the US population, access to accurate information aggregated from multiple data sources, such as longitudinal patient records, social determinants of health, immunizations, lab results, and the like, are critical when synthesizing comprehensive views of diseases and public health response initiatives.
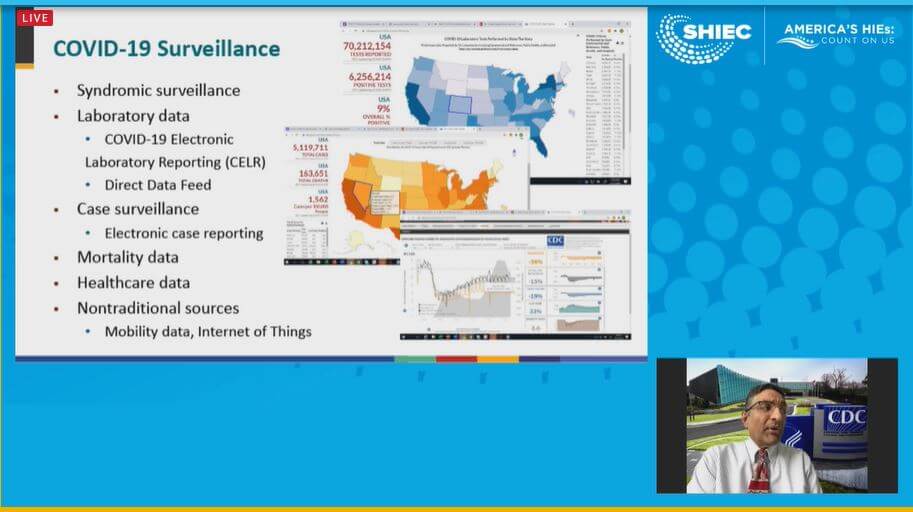
Dr. Gundlapalli outlined several key areas where we have experienced important improvements:
- Expanding the role that HIEs can and do play in solving interoperability limitations between major providers and public health information systems
- Championing and offering application standards to facilitate easier exchange and rapid use of information
- Easing the reporting and analytics burdens on providers as well as public health agencies
- Enabling the ability to link patient identities across systems and increasingly larger geographies
- Merging disparate types of data into a more complete longitudinal record to help understand the effects of public health emergencies on longer-term healthcare services and the effectiveness of provider and agency interventions
One of the key roles HIEs can continue to play is identifying, capturing, combining, cleaning, and standardizing data in repositories capable of serving patients with their own information, providers, public health agencies, and researchers. The role of data stewardship at the regional level is certainly a cornerstone of the advancements yet to come.
SHIEC Achievement Awards

- Date: Monday, August 17, 2020
- Presenter: Sharon Muscatell, RN, VP Strategy & Collaboratives, SHIEC
- Overview: Every year, SHIEC recognizes members of the HIE community for their contributions across seven domains. We join SHIEC in applauding the work these fellow industry leaders continue to do to improve the lives of those touched by an HIE.
Advocacy and Government Relations AwardAnnie Harrington, Chief Legal Officer, CORHIO |
 |
Community Partnership AwardVermont Information Technology Leaders |
 |
Emerging Leader AwardChase Millea, In-House Counsel & Director of Regulatory Compliance, Health Current |
 |
Innovation AwardMyHealth Access Network |
 |
Leadership AwardOne Indiana HIE Consolidation Team |
 |
Quality AwardCRISP |
 |
Chairmans AwardDave Navarro, Solutions Architecture Director, Indiana HIE and MHIN |
 |
In Memoriam

Keith Hepp was a national leader in health information technology and worked as a consultant to many other health information exchanges (HIEs) around the country. In honor of him, Xavier University has created the Keith Hepp Scholarship Fund.
The Role of HIEs in Public Health

- Date: Tuesday, August 18, 2020
- Presenter: Don Rucker, MD, National Coordinator, Office of the National Coordinator for Health Information Technology (ONC)
- Overview: Dr. Rucker focuses on the value of HIEs in achieving provisions of the 21st Century Cures Act.
Dr. Rucker outlined three critical facets of the 21st Century Cures Act and their value to public health planning and response.
- Removing barriers to interoperability is essential work. While we have made great strides as a community of healthcare and HIE professionals, we still face resistance, concerns about HIPAA and privacy, and other reasons for not yet having full participation across the country. We are getting there, but it is important to augment the many useful conversations with policies that directly discourage information blocking. That is, to remove the barrier we experience when certain data sources show reluctance or unwillingness to share their data for the common good. The Cures Act, in part, seeks to help address that barrier and prevent the practice of information blocking.
- The Cures Act also encourages widespread availability of Application Programming Interfaces (API), and specifically, with the modifier “without special effort.” This statement means that HIEs and solution developers need to ensure that APIs are based on true standards that make transactions easier to repeat across solutions, not only for the provider and public health communities but also for patients who will need to be much more involved in managing their healthcare data and their care, in general.
- The third major provision of the Cures Act is TEFCA. Congress’ intent for TEFCA, based on provider feedback, is to standardize the systems used to bridge networks. Sequoia, the coordinating entity, is planning to produce a draft of the Common Agreement in early 2021, at which time that draft will move through the necessary review process. The driving force for this work is to put patients in control of their care and to do so by facilitating a competitive marketplace where the best of the ever-evolving technologies available to them are selected.
Due to their essential role in assisting with implementing standards, cleaning data, and their ability to help deliver the tools that democratize data for patients, HIEs are increasingly being written into federal policies.
 Policymakers must assess what is working, what is not, and be able to quickly detect changes in public health, healthcare delivery capacity, and the results of policy and interventions. Because HIE data is a value-add feature in the flow of data, as opposed to an add-on source of overhead and duplication, HIEs have a very important role to play as facilitators and accelerators in a competitive environment. As HIEs continue to improve data quality and availability, the country reduces its reliance upon stand-alone and siloed systems, which often introduce waste, duplication, uncertainty, and incomplete insights.
Policymakers must assess what is working, what is not, and be able to quickly detect changes in public health, healthcare delivery capacity, and the results of policy and interventions. Because HIE data is a value-add feature in the flow of data, as opposed to an add-on source of overhead and duplication, HIEs have a very important role to play as facilitators and accelerators in a competitive environment. As HIEs continue to improve data quality and availability, the country reduces its reliance upon stand-alone and siloed systems, which often introduce waste, duplication, uncertainty, and incomplete insights.
During the Q&A portion of the session, Dr. Rucker provided commentary on a number of topics. Some highlights included:
- We are now seeing examples of bringing a much broader group of stakeholders together to make the use of data more effective. One example is Emergency Medical Services initiatives, where medics in the field can now leverage HIE data to see COVID-19 test results for a patient and share information with hospitals before patients arrive through connections facilitated by HIEs.
- A major value-add for HIEs to consider is finding ways to offer to remove the reporting burden for providers. This relief could be in the form of registry reporting, dashboards to monitor high-risk patients, or state-level disease reporting and analytics. HIEs should engage with their public health leaders to discuss opportunities to improve real-time insights using the increasingly robust data that HIEs are capable of accessing.
- Technology now allows us to solve some of the problems that have plagued the healthcare community in the past and slowed some of the solutions we have known were possible. For example, smartphones have enough usage patterns to help identify someone even without commonly used demographics. This kind of savvy use of technology will continue to evolve and should help to address concerns such as handling consent in a consumer-driven healthcare economy. We will, however, still need to grapple with difficult topics like consent for minors.
The Power of Public HIEs to Deliver Optimized Adult Vaccinations to Safety Net Clinics

- Date: Tuesday, August 18, 2020
- Presenters:
- Joshua Barbour, Associate Professor, Moody College of Communication, The University of Texas at Austin
- John Clark, CIO, Central Health
- Leanne Field, Clinical Professor of Public Health, College of Natural Sciences, The University of Texas at Austin
- Vincent Fonseca, Adjunct Professor of Public Health, College of Natural Sciences, The University of Texas at Austin
- Michael Popovich, CEO, STChealth
- Moderator: Phil Beckett, CEO, Healthcare Access San Antonio (HASA)
- Overview: The panel presented their experience developing the VAC-OPT Project in Texas. The goal of the project was to address challenges associated with identifying under-immunized adult populations and assisting providers with immunization-specific clinical decision support.
Texas leads the country in uninsured residents. The collaborators for the VAC-OPT project began by assessing gaps in information that often leads to manual processes and potentially unnecessary thinking time on the part of care team members. For example, pharmacies are a critical piece of the care ecosystem and administer vaccines. Thus, pharmacy data is vital to pull into patients’ longitudinal records to understand where and when they got certain vaccines.
Automating the inclusion of pharmacy-provided vaccination data can help providers eliminate uncertainty about vaccination history and extra steps to ascertain that history, or simply having to rely on patients’ memory. Adults often have a more difficult time remembering or accessing their own vaccination records. While there is often significant attention paid to immunizations for children, the percentage of adults staying current with immunizations is small.

There are added risks for under-immunized adults, such as co-infection. Adults who are not immunized and become infected with certain preventable diseases may become susceptible to other (also preventable) conditions. By bringing immunization information to the forefront for providers, the VAC-OPT Project sought to improve prevention efforts, which, aside from tobacco cessation programs, is one of the few initiatives we can undertake to provide significant upfront and near-term savings for the communities we serve.
Clinical decision support solutions work best when information and alerts arrive on time, are trustworthy, and are incorporated into clinicians’ normal workflow. When a patient has a vaccine administered at a pharmacy, and that information is combined with their previous immunization history, clinicians begin to see a clearer picture of risk and prevention opportunities to discuss with their patients. And when that information is presented to clinicians in their preferred medical record solutions as part of their standard workflow, clinicians are more productive and accurate, and patients stand a better chance of maintaining optimal health. Panelists discussed the hope that this model could be used across the country.
Perhaps even more essential to the program than technology was communication. The panelists discussed the critical role of relationship-building and engaging the pharmacy community and others to build this type of information solution. While the technology certainly exists to make it work, the conversations and collaborations rely heavily on identifying strong and effective conveners to help design a solution like VAC-OPT. It is essential that each participating entity feels that they are gaining something from the collaboration.
The session concluded with panelists talking about the value of being able to contact patients proactively when immunization opportunities are identified to improve prevention efforts, the strong financial incentives associated with preventing illness where possible, and the need for this type of information to be tracked at the state level or more broadly for best results.
Overcoming the Thorny Data Challenges of COVID-19: How 3 HIEs Guided Crisis Response Efforts
- Date: Tuesday, August 18, 2020
- Presenters:
- Kim Chaundry, Senior Director, HIE & Interoperability, Keystone Health Information Exchange (KeyHIE)
- Cody Johansen, MPH, Director of Operations, UHIN
- Anh Nguyen, PhD, MSPH, Director of Analytics, Nebraska Health Information Initiative (NEHII)
- Moderator: Daniel Cidon, Chief Technology Officer, NextGate
- Overview: Leaders from KeyHIE (Pennsylvania), UHIN (Utah), and NeHII (Nebraska) presented examples of their HIEs’ rapid-response COVID-19 solutions.
KeyHIE’s Kim Chaundy provided an overview of the dashboard content developed for their members and the state to visualize the spread and change of COVID-19 in the counties and communities where KeyHIE’s members operate. KeyHIE’s dashboard displays included maps showing COVID-19 tests, positive results, and spread or change in near real-time, as data became available to the HIE. Specific data elements included lab results by age category and county, as well as facilities where COVID-19 activity was increasing. This data was updated approximately every two hours and also included state-level views of available beds and the number of ventilators in use.
KeyHIE used their data to report on age, gender, race, and ethnicity statistics to show not only where and how quickly COVID-19 cases were identified geographically but also details like the higher rate of positive test results for women and certain race or ethnic groups.
In response to state requirements, hospital staff had been keying in capacity and usage information to support state-level insights at least three times per day. KeyHIE worked with those staff to automate reporting and relieve that particular burden. KeyHIE’s dashboards are still in use, and the KeyHIE team is working with both the state and its members to refine their tools and offer additional opportunities to drill into available data. Chaundy highlighted the fact that all of this was built on infrastructure that KeyHIE should put in place over the past many years. It was encouraging and exciting for KeyHIE to be able to quickly produce valuable insights to share and support provider and agency responses to COVID-19. KeyHIE continues to look for new opportunities to expand its value-add capabilities for the future. Chaundy also noted that she believes it will be valuable in the future for data to flow multiple directions. For example, both to and from state repositories.
UHIN: Cody Johansen presented a set of dashboards and metrics that UHIN developed to assist decision-makers in assessing changes and opportunities in COVID-19 policymaking and response efforts. In addition to capacity metrics, Johansen discussed the importance of drilling down into the different types of coronaviruses and ensuring that only results for the types relevant to this particular pandemic were used. As was the case in KeyHIE’s experience, UHIN was able to leverage existing infrastructure and data to craft information displays for its stakeholders and do so quickly. A key takeaway from this presentation was Johansen’s reminder that HIEs need to invest in infrastructure and highly flexible solutions to present information for rapid deployment well before a public health emergency surfaces. Johansen also mentioned that while UHIN saw a steep reduction in certain patient message volumes, there was no reduction in usage or viewing patient information among end-users and stakeholders. These actions signal consistent demand for HIE data, even when data quantity is diminished.
NeHII: Anh Nguyen offered a similar story in Nebraska. Fortunately, the state government in Nebraska backed NeHII’s data gathering and provided top-down support to encourage participation and use of NeHII’s infrastructure and tools for COVID-19 response activities.
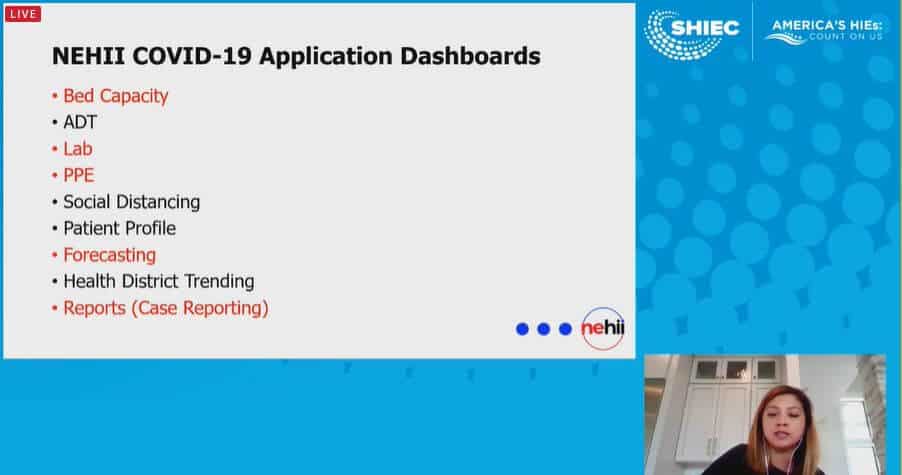
NeHII’s approach to visualizing statewide bed capacity was to combine ADT information with bed rosters from participating facilities to calculate real-time occupancy and bed availability. NeHII also developed dashboards specific to lab activity, ventilator use, and use by COVID-19 patients, in addition to forecasting dashboards to project PPE, ventilator, and bed needs.
Ayn discussed the critical need for NeHII to narrow the focus of stakeholder conversations. Because of the significant complexity in this pandemic response, in addition to every other initiative and solution an HIE might be delivering, it is paramount to distill conversations and direct stakeholders to the smallest number of high-value metrics, views, or questions that need to be answered. As we heard in other sessions so far this year, effective communication is seen as just as important, if not more important, than the technology or final solution design. Focused discussions are crucial to delivering rapid and effective solutions like these.
All three speakers talked about their organizations’ plans to continue monitoring and refining their dashboards and metrics through identifying and filling data gaps as states, schools, and other establishments are poised to re-open. Importantly, HIEs are focused not only on COVID-19 cases now but also in setting up appropriate monitoring tools to observe and report on possible longer-term effects of the disease, in terms of use of healthcare services, trends in health care conditions potentially attributable to former positive COVID-19 test results, and the effects of policy changes at the state level over time.
Part 1: HIEs Role in a Pandemic: Supporting the Healthcare Community

- Date: Thursday, August 20, 2020
- Presenters:
- Morgan Honea, CEO, Colorado Regional Health Information Organization (CORHIO)
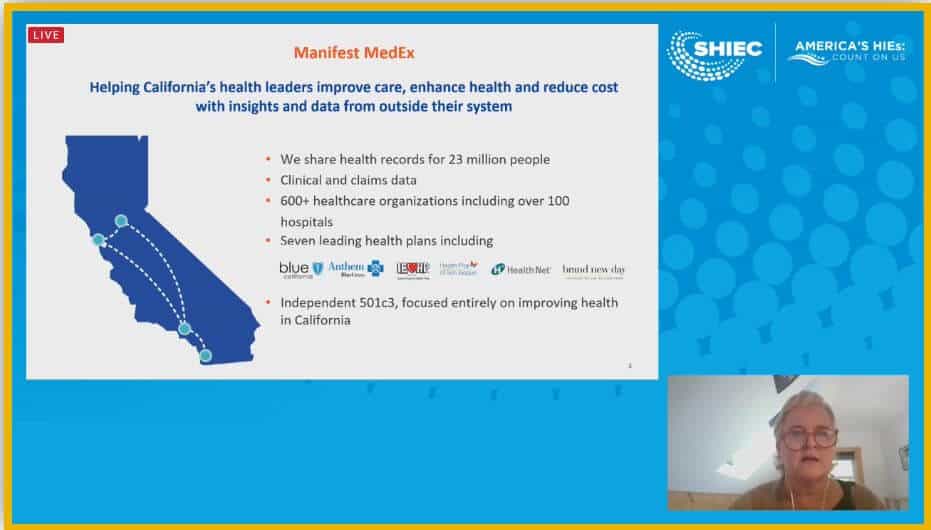
- Claudia Williams, CEO, Manifest MedEx
- Jaime Bland, CEO, Nebraska Health Information Initiative (NeHII)
- Overview: Leaders from Manifest MedeEx (California), NeHII (Nebraska), and CORHIO (Colorado) discussed what HIEs can do at a state or community level during public health emergencies like a pandemic.
Claudia Williams (Manifest MedEx) opened the session by describing some of the challenges states face when trying to respond to a public health emergency. States need data to inform multiple aspects of their day-to-day response plans. They require visibility into the affected populations, as well as the systems and infrastructure in place to support those populations.
In some cases, states have to deal with data coming to them from multiple, fragmented, or siloed sources, resulting in the duplication of data, multiple submissions of the same information that does not link together or merge, missing identifiers, or other data quality problems. These issues make it very difficult to say with certainty what is happening, changing, or improving as response efforts are underway. HIEs can make themselves essential to state and public health agencies by committing to cleaning data as a staple of what they do.
 Manifest MedEx has invested in analytics tools and processes over the years, enabling them to quickly adapt and create data products to help stakeholders. In one example, they created a COVID-19 screener that allowed payers to identify high-risk patients and contact them proactively, helping mitigate the risk of exposure to COVID-19.
Manifest MedEx has invested in analytics tools and processes over the years, enabling them to quickly adapt and create data products to help stakeholders. In one example, they created a COVID-19 screener that allowed payers to identify high-risk patients and contact them proactively, helping mitigate the risk of exposure to COVID-19.
Williams also discussed the importance of “policy accelerants” and policy barriers. Specifically, she talked about the need for HIEs to be involved and actively working to support more incentive programs encouraging participation in HIEs (such as 90/10 funding) and directly address barriers of this participation, such as resistance to sharing certain kinds of data. She stated that now is an excellent time for HIEs to invest heavily in engaging state legislators and building strong relationships. HIEs can help educate state and Medicaid leaders about the data that their organizations have available or can get, as well as can guide those conversations to identify opportunities to solve difficult problems for those leaders.
Jaime Bland from NeHII described the importance of HIEs assisting in advancing interoperability from a policy perspective. HIEs are uniquely situated to help articulate examples of cleaning and merging new combinations of data that produce valuable insights never before available to decision-makers. In order to do this well, however, we must have policies that accelerate and support growing these capabilities. Where we run into conflicting policies or barriers where certain policies could help, we need to invest in advocacy to pave the way to the future we would like to see.
Bland described the dashboards NeHII built to assist statewide COVID-19 response efforts and the success they had in doing so. That success was due to state-level support and engagement, as well as because of favorable existing infrastructure.
Morgan Honea echoed Williams’s recommendation to focus on relationships with policymakers and public health officials. Honea described CORHIO’s investment in advocacy and stated that it is an essential part of the future of HIEs. Really understanding the needs and pain points of stakeholders, addressing those needs at the HIE level, and then taking those stories to state and national leadership has been a significant part of CORHIO’s strategy for demonstrating value.
The Q&A portion of the session featured the following topics:
- State representatives should currently be on recess and available to talk about COVID-19 stories. Now is a good time to reach out if you have not already done so.
- It is essential for HIEs to work on streamlining access to disparate data sources, including pharmacy data, PDMP, and Social Determinants of Health (SDOH). HIEs need to combine this data and find ways to make it easier to access it in their area, especially if other states or regions already have it. HIEs also need to build a more consistent network of the same data to produce the most value for a highly mobile society.
- The panelists discussed the role of HIEs as a “health data utility.” Utilities are often situated between a resource and consumers, and while this concept makes sense, it causes us to think about leaning in the direction of making HIEs essential to public health efforts as a viable financial future. Everyone should look in this direction and make plans accordingly. It will be far more efficient and cost-effective for everyone if we find ways to leverage existing infrastructure rather than start from scratch to build stand-alone public health solutions.
ONC FHIR at Scale Taskforce (FAST): Scalable FHIR Infrastructure for Better Data Exchange
- Date: Thursday, August 20, 2020
- Presenters:
- Meena Jambulingam, Senior Director, co-lead FAST Identity Tiger Team, Optum
- Patrick Murta, Solutions Architect Fellow and Chief Architect of FAST, Humana
- Brett Stringham, Principal Information Security Architect, co-lead FAST Security Tiger Team, Optum
- Sandra Vance, Director of Healthcare Interoperability, AEGIS
- Overview: Members of the FHIR at Scale Taskforce (FAST) presented their progress in establishing and securing a pathway for FHIR to serve the needs and performance demands of a growing network of users.
The ONC FAST initiative seeks to develop plans for scaling FHIR solutions at a national level. This initiative is an ONC program with multiple teams working on different aspects of scalability.
Central to the topic of scalability is mastering patient identity at a national level. There are a number of barriers, including the variability in matching algorithms and criteria used locally and across regions, the use of different identifiers, and problems associated with relying on member rosters and attempting to reconcile such files on a national scale. The identity team is contemplating proposed approaches to standardizing patient matching and identity management that takes these challenges into account and still allows for both flexibility and the introduction and enforcement of standards. For these reasons, the identity is currently viewing their role, not so much in terms of offering a single solution, but in providing a maturity model through which organizations can work to achieve higher levels of patient identity standardization.
The security team is primarily focused on the measures necessary to enforce “trust” in any given solution. This focus will likely mean third-party attestation capabilities and the concept of a portable identity for authentication purposes. The security team is also concentrating on limiting the data transacted to only that which is appropriate for the given transaction. This limited data transaction is in contrast to previous models where “all available” data is sent or viewable, such as in the form of a CCD or C-CCDA. While useful, the team believes that narrowing the amount and scope of data delivered and accessible to only what is needed is a critical part of a scalable security policy.
Presenters outlined a series of steps to rapid FHIR scalability, including specification conformance validation, infrastructure use case certification for component parts of FHIR transactions, and functional use cases with key partner organizations to demonstrate in practice.
ONC’s work includes establishing testing and certification recommendations, as well, which are likely to require an automated testing platform for structured steps of FHIR transactions. Base FHIR validation would be required as part of the ONC FAST certification program. Once FAST certified, organizations will be guaranteed to be interoperable with other ONC FAST Certified systems. The certification program will be further refined as the work from the other FAST teams complete their designs and recommendations.
For more information about ONC’s FHIR at Scale Taskforce and the taskforce teams’ proposed solutions, please visit their page.
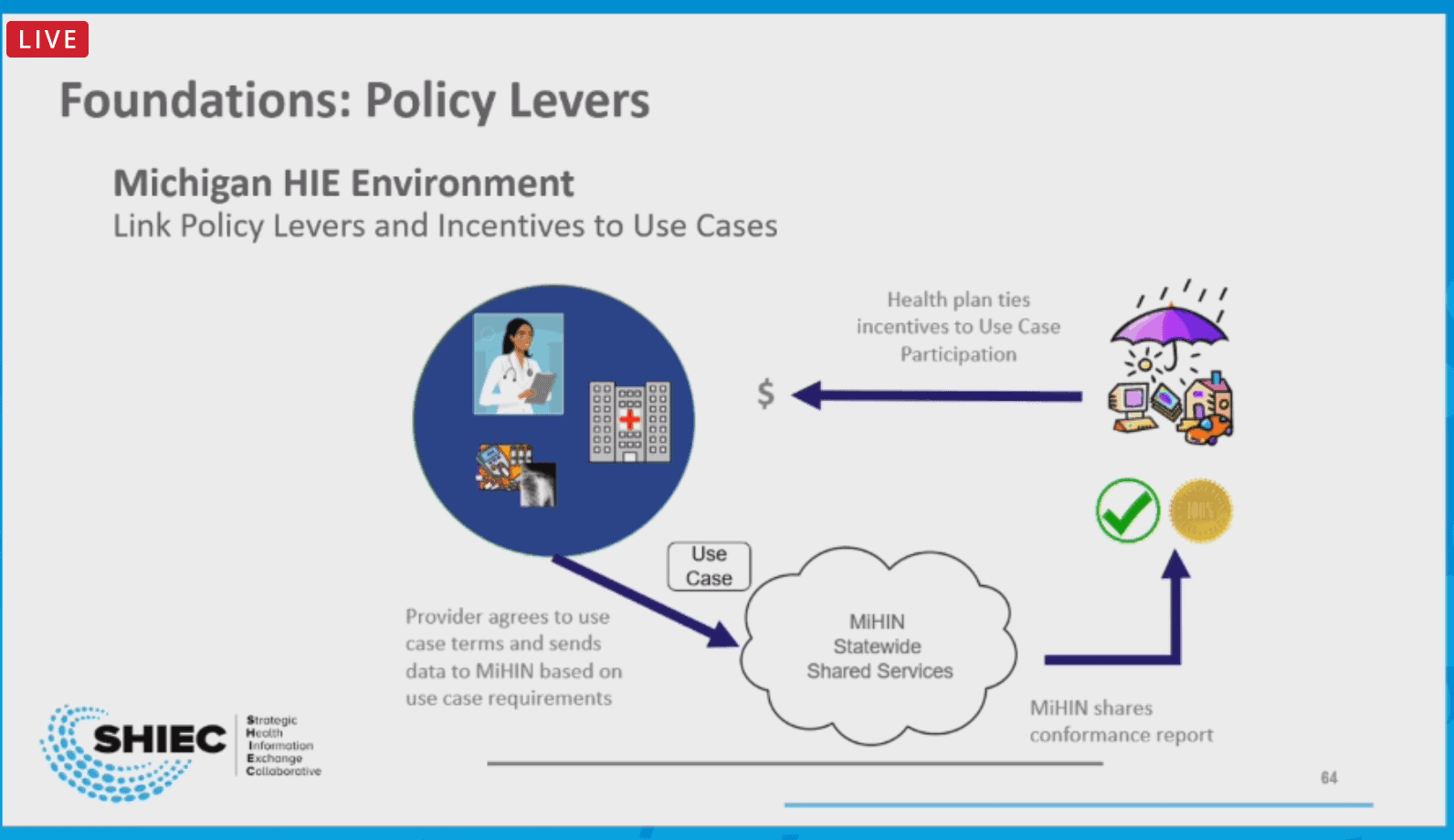
Strengthening Patient-Provider Connectivity with “Telehealth 2.0” and a Look Ahead in Texas
- Date: Thursday, August 20, 2020
- Presenters:
- Chris Bailey, Director, National Engagement & Consumer Health Strategy, Michigan Health Information Network Shared Services (MiHIN)
- Phil Beckett, CEO, Healthcare Access San Antonio (HASA)
- Sharon Kim, Senior Health Care Analyst, Blue Cross Blue Shield of Michigan
- Tim Pletcher, Executive Director, Michigan Health Information Network Shared Services (MiHIN)
- Overview: HASA, MiHIN, and Blue Cross Blue Shield of Michigan described how they partnered on an innovative project to deliver telepsychiatry visits for foster care children.
BCBS of Michigan has a long history of developing incentive programs and partnering with stakeholders in Michigan to improve access to care and expand progressive types of services available to their patients. The company has invested in telehealth and other incentive initiatives to increase participation and adoption of emerging and process-consolidating technologies.
Telehealth took on a new level of urgency as the COVID-19 pandemic began to take shape, and BCBS of Michigan and its partners were positioned to respond. Within two months and with the support of incentives, participation surged across the state. Efforts have focused on BCBS of Michigan’s Physician Group Incentive Program (PGIP), which now has 100% participation across 40 physician organizations and approximately 2,000 offices across the state.
Program leaders are actively pursuing strategies to empower patients to self-activate engagement with the healthcare community and use flexible technologies to take a greater role in managing their care. Telehealth platforms provide a useful platform to facilitate that kind of engagement. Multiple speakers have noted that essential technologies are now in place, including telehealth capabilities, but there is a call to the community to find new ways to use it.
For example, care can become much more immediate, with potential improvements in reducing lags. ADT messages not only move between integration engines and provider solutions, but can now be leveraged for real-time notifications, monitoring, and even triggering phone calls or on-demand virtual visits the moment ADTs arrive with qualifying details. This level of care, facilitated by advanced technologies, enables care team members to swiftly intervene and guide patients instead of missing prevention opportunities or waiting for their problems to worsen.
The presenters believe that consumer access to more of their data from a variety of places will help to empower individuals to take a greater leadership role in their care and cost-saving preventive measures.
The high availability of smartphones and stable communication networks now afford us opportunities to put tools in front of consumers that make a difference, both in terms of clinical effectiveness and reducing administrative burden. One such example is providing telepsychiatry visits for children in the foster care system.
In this model, children in the foster care system who relocate are required to have a behavioral health visit. Superior HealthPlan in Texas, which runs a health plan specifically for foster children, provides an attribution list to the HIE in Texas (HASA), which then cleans and matches data and facilitates data exchange to and from Pine Rest, whose providers deliver the telepsychiatry services. Data about the visits is then sent back to Superior HealthPlan for reimbursement to the PCP and Pine Rest for their services. This program is financially sustainable and highlights the importance of HIEs looking for creative ways to solve problems, even if the answers to those questions can be found across borders.
The presenters mentioned that this example is a good pilot for a specific population, but can certainly be expanded for a variety of other patients. The value proposition includes patients having their visits virtually in a convenient location, the PCP and telepsychiatry providers receiving compensation for their time and services in an efficient way, the health plan receiving important information that can be used for outreach and additional preventive services, data sharing becoming automated and efficient, providers engaging in a system that can be used for more of their patients beyond those in the foster care system, and the HIE anchors itself being an essential component of the data transaction pipeline. This proposition, indeed, is part of the promise of HIEs moving forward: the ability to connect parts of the marketplace that have previously been unknown or inaccessible to one another. We encourage everyone to continue to think creatively about what local problems your HIE can go out and find solutions to address.
Thank you for joining us this week at SHIEC!
| Week Two Summary | Week Three Summary | Week Four Summary | Week Five Summary |
|---|
J2 Interactive is an award-winning software development and IT consulting firm with a specialty in customized solutions for HIEs. Read about HIE platform migration.
We would be happy to have a no-obligation discussion about your HIEs needs with you.
